Radiofrequency Ablation for Treating Uterine Fibroids

With the recent increase in both patient and provider education, women with symptomatic uterine fibroids have been shifting their treatment choices away from open, abdominal surgery toward safer, less invasive methods. Radiofrequency ablation (RFA) is one of them.
What Is RFA?
RFA is a minimally-invasive, non-surgical procedure in which a slender needle with an electrode is inserted either through your vagina or through a tiny incision in your abdomen. Guided by ultrasound, the electrode is inserted into the fibroids. The heat from radio waves sent through the electrode kills the fibroid tissue. The fibroids shrink, and the dead tissue is reabsorbed into your body. Normal tissue in the uterus is not affected by the energy waves.
Since no tissue is actually removed from your body, your surgeon will first make sure that there is no risk of any of the tumors being cancerous (leiomyosarcomas). According to Dr. Jen Mushtaler of the the Kindbody clinic for women’s reproductive health, this is determined by:
- An in-depth family history
- How fast the tumor has been growing
- Findings on imaging tests
- A Pap smear
- A biopsy
The RFA procedure itself is performed under general anesthesia, and most patients go home as soon as the anesthesia wears off, usually in a couple of hours. If an incision was made, then a Band-Aid will be placed over the site.
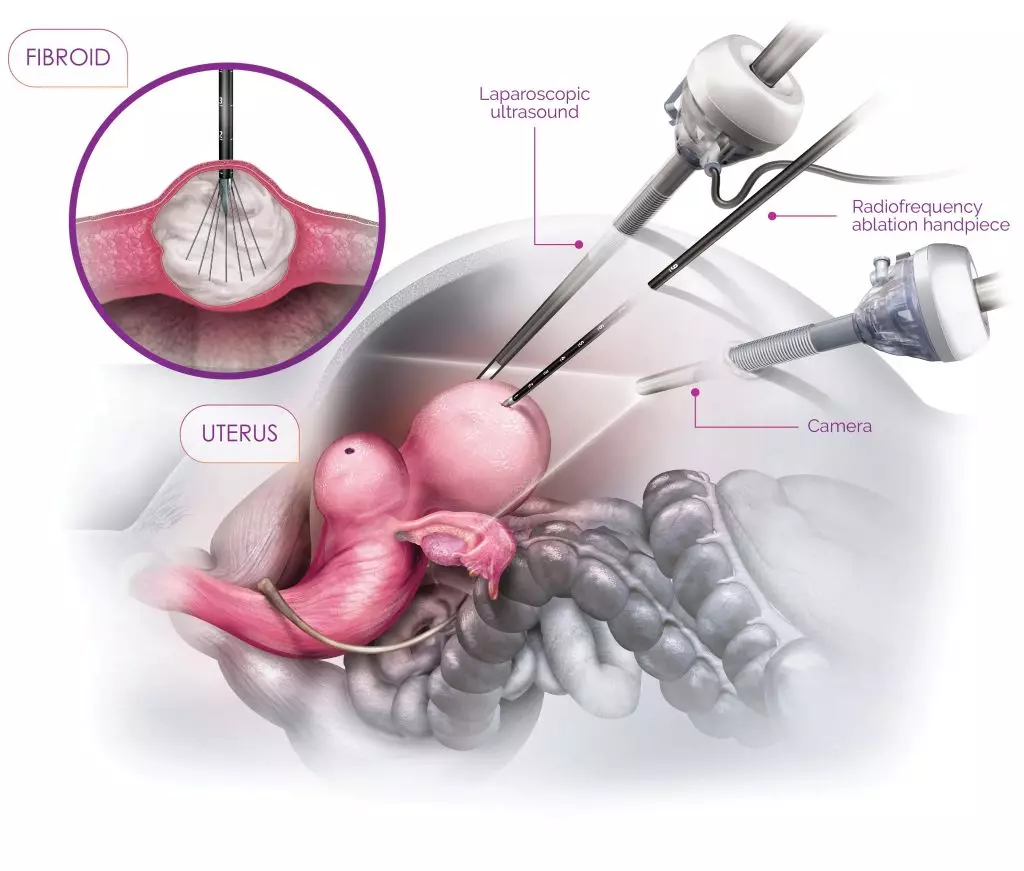
This diagram shows the Laparoscopic RFA procedure
(This image is from Contemporary OB/GYN.)
Are you a good candidate for RFA?
The location and size of your fibroids are primarily what determine whether or not RFA may be a good treatment option for you. For instance, Mushtaler says, fibroids that grow inside the uterine cavity (submucosal fibroids) do not tend to be responsive to radiofrequency. A better option for treating those fibroids, she says, may be to have them removed by hysteroscopy.
Fibroids that grow on the outside of the uterus on a stem (pedunculated subserosal fibroids) are also not optimal for RFA, Mushtaler says. She recommends that patients explore myomectomy to remove those fibroids.
Larger fibroids–those over 5 cm in diameter–can prove challenging with RFA, because the larger the fibroid, the more difficult it is to ensure that all the fibroid tissue is adequately treated. Some patients with large fibroids may be left with bleeding issues and other symptoms.
The fibroids that respond best to RFA are those that grow inside the thick uterine wall (intramural fibroids) and that are no larger than 2 to 5 cm in diameter. These, says Mushtaler, “respond quite favorably,” adding that a very high percentage of her patients report that their symptoms are completely resolved.
Speak with your doctor about the size and location of your fibroids, along with the pros and cons of RFA treatment for your unique fibroid situation. As Mushtaler says, “Not all fibroids are equal.”